2:23 pm
September 26, 2025
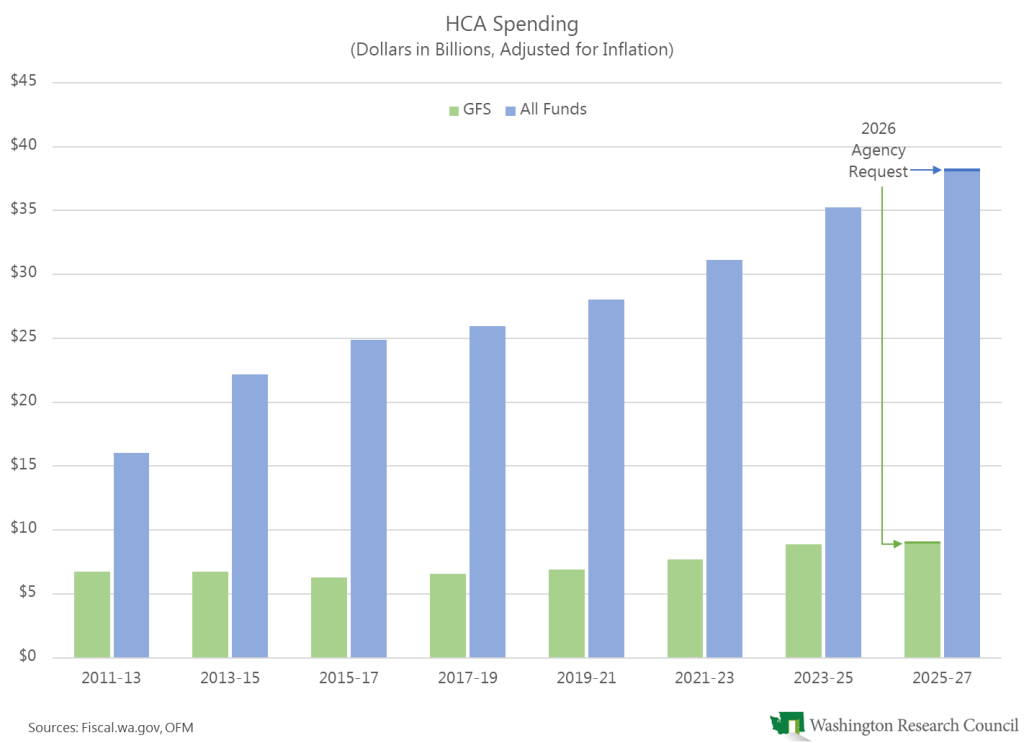
The enacted 2025–27 operating budget appropriates $8.924 billion from the general fund–state (GFS) for the Health Care Authority (HCA). For the 2026 supplemental budget, HCA is requesting an additional $201.0 million (2.3%) from the GFS for the biennium. The additional spending would cost $267.9 million in 2027–29. Most of this GFS impact comes from two items:
- $142.0 million to restore Medicaid program integrity savings. The 2019–21 budget required HCA to implement program integrity efforts, and that budget assumed that the state would save $101.8 million in 2019–21. (The HCA request notes that program integrity efforts are “federally mandated to prevent, identify, and investigate potential fraud, waste, and abuse” in Medicaid.) Apparently, the underlying base funding for Medicaid in the state budget was adjusted to assume $142.0 million in GFS savings each biennium from program integrity efforts. These savings have not been realized, and previous budgets provided funding (at the policy level) to restore the assumed savings ($32.6 million in the 2020 supplemental, $71.0 million in the 2021 supplemental, $142.0 million in the 2021–23 biennial, $35.1 million in the 2023–25 biennial, and $107.0 million in the 2024 supplemental). The 2026 budget request would restore the savings on an ongoing basis.
- $38.2 million in 2025–27 and $72.6 million in 2027–29 for 23-hour crisis relief centers. According to the request, non-Medicaid utilization of these centers “is more significant than the original fiscal assumptions.”
Another major request would indirectly impact the GFS. HCA requests more funding for Cascade Care, which is the state’s premium assistance program for Washingtonians with income up to 250% of the federal poverty level who purchase health care through the Health Benefit Exchange. The proposal would provide $65.0 million in 2025–27 and $260.0 million in 2027–29 for this purpose from the state health care affordability account. However, this is really a GFS request because the money in the health care affordability account comes from GFS appropriations. From 2021–23 to date, the state has appropriated $250.0 million from the GFS to the health care affordability account. Current funding will last either through 2025 or 2026. (The 2025–27 budget documents say the program is funded “through calendar year 2026” but the HCA request says that the program is funded “through December 31, 2025” and, later in the document, “through the 2026 calendar year.”)
All told, the request does not provide a good estimate of the maintenance level (the cost of continuing current services, adjusted for caseloads and inflation). Instead of using the June caseload forecast (like DSHS did), HCA is waiting for the November caseload forecast, and its request does not assume any changes to caseloads or utilizations since the budget was enacted. (A placeholder request related to H.R. 1—the federal legislation that makes several changes to Medicaid—notes that various provisions of the bill are “expected to have a negative impact on HCA’s caseload. The Caseload Forecast Council . . . is currently working on incorporating these changes into their official forecast.”)
As I’ve written, the impacts of H.R. 1 on Washington’s budget are not clear. The HCA request includes a placeholder addressing H.R. 1. Specifically, the request would implement the administrative changes required by H.R. 1 (e.g., six-month eligibility periods) and fund maintenance and operations of the Master Person Index. HCA writes that it “anticipates significant administrative fiscal impact from H.R.1. However, the magnitude of the impact is currently indeterminate because it depends on the implementation plan. The implementation details are in the process of being finalized within HCA and in collaboration with other affected State agencies.” A separate placeholder asks for spending authority for any federal funds allocated to Washington for rural healthcare under H.R. 1.
Finally, the request includes a placeholder regarding the hospital safety net assessment program (HSNP). Beginning in 2010, the state has levied an assessment on hospitals and returned the collections to providers as Medicaid payments, generating the federal Medicaid match. According to the HCA request, legislation enacted in 2023 “increases both the amount of funds collected by the assessments and increases the total amount of funds provided to hospitals from the HSNP. Current appropriations do not align with projected expenditures.” HCA wants to continue the program, but HCA is waiting for the November caseload forecast before providing a cost estimate. The placeholder request makes no mention of the changes in H.R. 1 that limit state Medicaid provider taxes. It’s not clear if the federal legislation affects this request.
(Previous posts on the 2026 supplemental budget requests are available here.)
Tags: 2026 agency requests